In a recent radio programme, a group of workers lamented the fact that black youngsters did not have role models and might be suffering a number of difficulties because of this. In a brief moment the general problem was identified but there was a sense of hopelessness regarding the solution. The specific question is whether widespread problems exist among now distant descendants from the grim history of African slavery in the Americas and the Caribbean.
By presenting an historical overview we are able to witness the stark realities of a migrant population better understood by its fractured interpersonal relationships and struggle to maintain an inherent dignity and semblance of its own identity.
As such, I will attempt to discuss the issues leading to the introduction of the inhumane and brutal system of African slavery and the difficulties encountered by subsequent generations in overcoming (or recovering) from this tragic set of circumstances. I shall contend that it is the cumulative effects of the traumatic injury prior to coming to Britain that has sought only to compound an already fragile migrant psyche. This vulnerable group, having suffered rejection and exclusion in Britain, manifest in the high rates of behavioural and mental disorders.
Britain has been involved in the lives of Caribbean people for around 360 years, but the extent of this involvement has not been consistent from country to country: in Jamaica and Barbados the involvement was almost total; in Trinidad and Tobago and several other islands in the Eastern Caribbean, the British and French alternated as rulers; and in Guyana, South America the Dutch were dominant for much of the time prior to emancipation (freedom) from British slavery in 1833. It is of interest to note that Jamaica (population of 2.8 million, represents half the regional total), is 1100 miles away from the other main population group in Trinidad and Tobago and a further 350 miles from Guyana.
Before emancipation
Prior to emancipation the institution of slavery paid little regard to human life or custom. There was no contact between Caribbean people and their African forefathers and efforts were made to eradicate all aspects of Africanisms among the slaves.
Slaves were property to be sold or bought (chattel) and to be regulated. Mating behaviour was dictated by those running the estates. Women were not accorded any greater respect than men, and evidence suggests that they were subjected to very high levels of abuse and exploitation.
Following emancipation, the British recruited indentured (contract) workers from China initially, then small numbers from African countries, the Middle East from Syria and Lebanon and from Ireland and other parts of Europe. Large numbers of South East Asians settled in Guyana and Trinidad and now makeup around half of the populations there.
In the post emancipation period, many of the economies have long since declined and the population experienced great difficulties in their quest for security and stability. Many descendants of ex-slaves and the white master-class migrated to Central American countries, Cuba and USA to seek work in this period. The peoples in Caribbean countries were largely unknown to each other before migrating elsewhere. The majority had been brought up in settings in which the African mask (slave tradition skin colour, language and religion) was despised, ridiculed and a source of great shame.
It was against this backdrop that an unprepared and largely deprived migrant population arrived here in Britain, facing difficulties far greater than anyone might have predicted. These were associated with high levels of rejection - at work, in housing, in schooling and childcare and in everyday life. With the passing of time it may be true to say that these wounds might have healed, but if so, this raises a number of questions:
- What were the cumulative effects of traumatic injury?
- What was the likelihood that the population choosing to migrate did so at random?
- Were the expectations of this population based on their beliefs in belonging to the ‘mother country'?
Some time ago, I carried out a follow-up study of patients repatriated to Jamaica because of mental illness. Evidence suggested that the great majority did not use English as their first language and only ten per cent of those migrating to Britain in adulthood gave a history of attending a secondary school. Most came from poor backgrounds and could be described as highly vulnerable.
These findings indicate that the migration to Britain was heavily weighted in favour of deprived and vulnerable persons, rather than the more established and socially aware. Reports suggest that Caribbean migrants to the USA and Canada have enjoyed a better fate than their British counterparts. Migration to Britain was associated with both return migration home of vulnerable persons and others as well as re-migration elsewhere of the more robust.
Origins and nationalities
It is unclear where best to place the African Caribbean people in terms of origins and nationalities. The European historical link runs hand in glove with the African but the two were on different levels. This duality in background becomes a source of conflict among these much displaced groups of individuals identified by orientation, language, history, church attendance and socio-economic variables. The conflict may be acted out or it could remain dormant or hidden or indeed may be experienced asbeing quite marked and the basis for a psychological disorder.
In Caribbean countries, African and Asian ethnic groups are considered to be separate, with one group adopting the religion and style of the owner class, whilst the other retains its strong cultural and religious links with ‘Mother India'. The former is encouraged to deny its African background and instead to seek to be British or American. The contradictions in this journey are all too obvious.
Researchers have argued that research methods should be employed in quantifying the extent of racism and the consequences of this among different groups. Some take the view that, despite disparate Caribbean styles and country histories, it is not unreasonable to include these groups as members of one ethnic group by virtue of British slavery and colonisation.
In the USA, researchers have pointed out that in this ethnic group designation of a similar population, there is employed as a proxy of deprivation and disadvantage with knock on effects of further stigmatising the group by adverse research findings. It is likely that Caribbean migrants to Britain were of the opinion that they were moving from one part of the Empire to another and would have been treated as equals and not rejected.
Theories
Sociological and psychological theories do not explain the very high rates of behaviour (conduct) disorder among black youngsters the USA, in South America, the Caribbean, and Britain and elsewhere in Europe. Anomie theory may to some extent explain rates of deviant behaviour among racial groups in the USA and these theories are unlikely to explain findings here in Britain. The fact is that African American and African Caribbean people suffered profound displacement in slavery and subsequently as well.
Attachment theory attempts to provide a framework for explaining the extent to which human behaviour will be modified by faulty relationships between caregivers and their offspring in early life. The history of European slavery in the Caribbean provides a reservoir of material on this issue. It is unlikely that secure attachments (cf. insecure attachments) were prevalent among slaves.
Some have argued that attachment theory may help to explain the effects of traumas suffered by children left behind in serial migration from the Caribbean and joining their parents later on. This might explain the high levels of mental disorders among the second-generation who migrate in adolescence. It would also explain the finding that delinquency among African Caribbean youngsters in Britain is associated with multiple separation experiences from carers in early life.
Theories on the role of adversity in psychosis might suggest that the group of individuals migrating in adolescence will be doubly loaded in terms of loss and adversity. Evidence suggests that members of the group display high levels of anxiety, irritability and depression and become victims in the classroom where they may be excluded permanently for disruptive behaviour. At a later age they are far more likely to be detained because of delinquent behaviour.
The experience of African Caribbean youngsters suffering from learning disabilities may be of interest; they seemed more likely to be accommodated in locked units than clients from other ethnicities. As the same is true for the less vulnerable sector of the population (not learning disabled) it suggests a tendency to label the population as ‘dangerous'. This may be the outcome of two groups responding to each other with the threatened group deemed to be aggressive and stigmatised because of this.
It is of considerable concern that rates of being ‘looked after' by local authorities might be up to five times greater for African Caribbean children than others. Statistics of this phenomenon have been consistent for many years, with little change in the proportion of children without a home and who are likely to experience life lonely and without support. It would be easy to argue that this situation is the responsibility of the families of these children and has little to do with the historical background. However, the fact is, that a secure base is acquired by way of a family structure in a community with its customs in rules and in the context of a country. If the concept of country of belonging is eroded then it is necessary to supplant this idea by creating another country. For many of the Caribbean people migrating here to Britain it is not unreasonable to suppose that they believed that the secure base was Britain. Instead the migration ensured that family structures would be destroyed with extended family members remaining behind and unlikely to be allowed to reunite with their migrant kin.
As indices of malfunction do not suggest that the long-term effects of stress and conflict among British-born African Caribbean residents have been reduced, in comparison with findings among secondgeneration migrants, it seems likely that the rates of behavioural malfunction and psychological disorders will continue to be significantly higher in the African Caribbean sector of society.
It should be of interest in passing that the small Asian Caribbean population living here in Britain have not had a similar experience as the African Caribbean group. Yet, it is unclear whether the selective factors leading to migration are different and whether the populations were likely to be exposed to different levels of stress; finally whether one group is more resilient than the other.
Behaviours
It is widely accepted that selfharm and suicidal behaviours are symptomatic of depressive syndromes, whilst physically violent behaviours indicate the likelihood of crime and not invariably a psychiatric disorder. Clinical practice suggests that the two behaviours are related to gender and ethnicity with an excess of suicidal behaviours among females and white British. The two conditions may co-exist with causation factors for the resulting three groups (separate and co-existing) in need of study. It is known that experiences of abuse, relationships with parental figures, the misuse of illicit drugs and the extent of psychotic disorders are important factors in all three conditions. It is not unusual for clients to become restless, unsettled and suicidal following loss or threatened loss (rejection).
Marked over-representations of African Caribbean clients are found on locked wards of mental hospitals, on special hospitals for the dangerous; in prison facilities, and among patients held by the police on emergency sections of the Mental Health Act. These findings may well be the outcome of how society deals with behavioural disorders whether or not these are associated with mental illnesses and indices of social exclusion. What does seem to be true is that findings of behavioural excesses among children and adolescents will be followed by similar findings of excesses among adults.
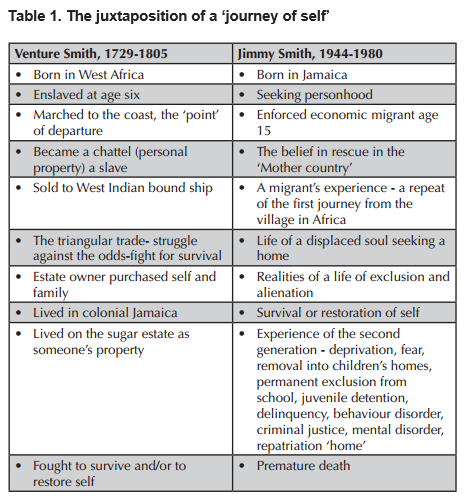
It would be important to consider the extent to which these findings might have been evident in the early stages of the experiences of Venture Smith and Jimmy Smith in their respective journeys from Africa and from the Caribbean (see Table 1):
Stark findings
Language is an important factor preventing meaningful communication between threatened and threatening groups; mistrust exists between these groups. One consequence of this mistrust might be the fear of black persons displayed by those in authority in facilities for mental disorder, and the criminal justice system. For some time now, the Institute of Race Relations has been monitoring deaths in custody whether in prison units, hospitals or elsewhere. The findings are stark, black youngsters mostly men are markedly overrepresented.
Some years ago, I visited a remote village in Jamaica to explore the possibility of the return home of a troubled young man incarcerated in a locked unit. Sadly he suffered an unpleasant death in that setting shortly after I returned to tell him of my findings. In that circumstance it is likely that the coroner's verdict would be death by misadventure or by accident. However, this verdict may not do justice to the combination of factors resulting from fear and mistrust between workers and clients. An appropriate label for this condition could be – ‘worker-client mistrust syndrome'.
In these circumstances the basis for both police intervention and mental health involvement may seem to be well established. However the merits of one form of intervention rather than any other remains unclear.Here in Britain, there has been considerable interest in the fate of the African Caribbean population diagnosed to be suffering from schizophrenia. This is often associated with criminal behaviour but this finding is far more likely among African Caribbean persons than any other group of patients. It is also true that police arrest and detention is far more likely among black and minority ethnic males than other groups.
Clearly three conditions can be distinguished by the nature of the resulting incarceration:
- Violent criminal behaviour (VCB) without hospitalisation
- Hospitalisation but no VCB - more likely among white patients
- VCB and hospitalisation
A study of the factors contributing to these three behaviours, and the resulting incarceration, may not reveal any differences in the distribution of causative factors. If this is so, it would suggest that the institution of criminal justice and the field of mental health are interlocked, and that this is true when the task concerns African Caribbean clients.
There is no good evidence of any ethnic difference in the distribution of commonly accepted forms of abuse in the causation of mental disorders or criminal behaviour.
However debate on the role of racism as a causative factor in these conditions has led to great dispute and conflict among practitioners and researchers. There can be no doubt that racism affects the lives of those who perceive these occurrences as well as those who have learned to live with this reality without raising the issue. The critical question will remain: whether racism may contribute to the excess findings of behavioural disorders and mental illnesses among African Caribbean persons in Britain? An attempt to answer this question should mean identifying an appropriate group for comparison.
Mental and behavioural disorders among the migrant elderly constitute a special group and might suggest the need for close monitoring of physical health in this age group. Workers in the USA take the view that the higher prevalence of hypertension and resulting stroke among African Americans than White Americans may be the outcome of stress related factors.
African Caribbean persons suffering from pre-senile dementia may be prone to behavioural disorders, but the extent of the problem is not known.
In concluding, we should consider whether the African Caribbean population in Britain should give some thought to the idea of whether it constitutes a group, and if it does whether changes in its function and organisation may be necessary. There are a number of relevant questions.
- What is the nature and extent of conflict between being black and being British in this population?
- What steps should be taken to overcome this conflict?
At an earlier stage of this discussion I made note of my visit to Jamaica to follow up a group of patients repatriated because of mental illness. It may be appropriate here to give some outline details of the outcome experienced by the several subgroups in that population:
- The carers – returned home because of their need to reestablish family links necessary for childcare. This group enjoyed a good outcome.
- The alienated – remained unsettled in Britain but did not suffer from severe mental illness. They did not enjoy a good outcome.
- The displaced – returned home following incarceration for mental illness associated with crime. The outcome was very poor.
It would be of some concern to know whether findings in that early study might be as relevant now, as then.
When patients present with symptoms of mental illness it is not always very clear whether the aims of therapy should be to protect the public or individual, or to achieve meaningful change in the patient's relationship with self or/and others.
Necessary conditions for change should be identified in order to achieve any of these goals. When faced with a client who feels displaced and alienated it would be important to include a community approach. I do not believe that it would be sufficient to attempt to overcome difficulties simply by counselling or psychotherapy or by way of incarceration. There is a risk that the situation will remain unchanged because of the feeling of helplessness in respective sectors of the community.
Dr Aggrey Burke is a Consultant Psychiatrist, and Trustee, George Padmore Institute