Suicide is a catastrophe for communities and families as well as for individuals. Policy makers who plan to reduce its likelihood deserve public support. They need to identify people at higher risk and to be aware of factors that can be positively changed. Effective policies should be informed by an understanding of lifetime risks, which includes taking fully into account childhood experiences. But who is at risk of contemplating suicide, and what are the factors that play a part? Here we analyse evidence about one such group – adults who as children have been in forms of care and, in particular, a children’s home, borstal or young offenders unit.
The placing of children in care is the outcome of adverse experiences. It acts as a marker of prior disadvantage. Being in care can be accompanied by feelings of neglect, fearfulness, or abuse. It often represents but one episode in a drawn-out process that diminishes the ability of individuals to cope with stresses and to make wise choices in adolescence and adulthood. An abundance of research suggests strong associations between having been in care and susceptibility to mental health, behavioural, and educational adversities in adulthood (Bruskas, 2008). Data from the second National Psychiatric Morbidity Survey (2000) revealed that early negative experiences were linked to the subsequent development of neurotic and psychotic disorders and of alcohol and drug problems in adult life (Bebbington et al., 2004). These experiences were more common in care leavers. Mental health outcomes in care leavers appear to be disproportionately poor in comparison to the general population, with the statistics speaking for themselves: in an American study, 50.6 per cent of people who had spent time in foster care had been diagnosed with a psychological disorder (Pecora et al., 2003; 2006).
A high prevalence of psychiatric symptoms, suicide attempts, conduct disorders, substance abuse and criminality has been reported in adolescents and adults placed in long-term foster care during childhood, compared with the majority of population peers among other groups (Berlin et al., 2011). Pilowsky and Wu (2006) found that such adolescents were four times more likely to have attempted suicide in the previous twelve months, and about five times more likely to have received a drug dependence diagnosis than the general population.
Child institutionalisation and suicide
In spite of the above, there is very little research on the association between a history of childhood institutional care and attempts at suicide and suicidal thinking in adulthood. In the study reported here we examined this question by using data from the latest National Psychiatric Morbidity Survey.
The Adult Psychiatric Morbidity Survey (APMS) was carried out in 2007 on a sample representative of the population of England, involving over 7,000 people. The interviews included structured assessments and screening instruments for mental disorders as well as questions about other topics. Information was collected about experiences of childhood institutional care. Binary logistic regressions were used to analyse the data and investigate whether there was a positive association between being in local authority care or a children’s institution and participants’ lifetime history of suicide attempts and ‘ideation’ (or thinking).
The results of the analysis showed that suicide attempts and thinking were both significantly related (odds ratios, respectively 5.1 and 2.9, p <.001) to the experience of being in a children’s institution, such as a children’s home, borstal, or young offenders unit. Local authority care was significantly associated with lifetime suicide attempts (p = .003), but not with suicidal thinking.
Children’s institutions
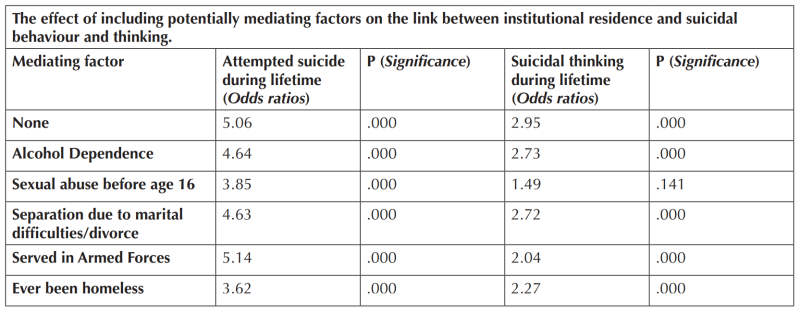
In the further analyses presented here we focus on those participants who had spent time in a children’s institution. Logistic regression is a form of analysis that allows the assessment of more than one factor on a given outcome. We used it to investigate variables that might mediate the association of institutional residence with suicidality. Mediation implies that the association may come about because of additional factors that are themselves associated with institutional residence, and that the latter operates through these other factors. Mediation implies that controlling for the mediator (i.e. introducing it into the analysis) should reduce the strength (the odds ratio) of the relationship between institutional residence and suicidal tendencies. Partial mediation reduces the original association appreciably, but does not render it non-significant, while complete mediation would make the original association nonsignificant.Findings in relation to a range of mediators are illustrated in the table above. They show that having been sexually abused before the age of 16 and experiencing homelessness are the most likely candidates for mediation. Sexual abuse before the age of 16 was the only factor to reduce a significant association to an insignificant one (the significance of the relationship for suicidal thinking was reduced from p=.000 to p=.141).
Findings
The primary purpose of this study was to test the hypothesis that there is a link between being in child institutional care and lifetime suicide attempts and thinking. Our results strongly supported this hypothesis. The potentially mediating variables used for this analysis were carefully selected as a result of preliminary logistic regression on variables from the 2000 Adult Morbidity Psychiatric Survey. The analysis presented in the table shows little effect of alcohol abuse, subsequent marital separation or divorce, or membership of the armed forces, despite the fact that these variables are all related to suicidality. The strongest candidate for mediation was sexual abuse. When introduced into the analysis linking suicidal thinking and residence in a children’s institution, sexual abuse reduced the association to statistically non-significant levels (.000 -> .141). It was not possible to date the abuse in relation to the period in care, and it could thus have occurred before, during or after it. Clearly some instances of care may follow the revelation of abuse. These results may nevertheless support previous research findings that link adverse experiences of care to a range of negative consequences for care leavers’ mental stability and health in later life (Berlin et al., 2011; Pilowsky and Wu, 2006). The experience of homelessness was the only other candidate mediating factor that strongly reduced the effect of the association, bringing the odds ratio for suicide attempts over a lifetime down to 3.62 from 5.96.
Implications
Childhood experiences are more than a series of temporary episodes, good or bad; their impact may be mortally wounding in the long term. To prevent such fatal consequences we should invest in services that are quick to recognise emotional damage and to promote long term recovery and care for all young people, in whatever kind of institution they happen to be placed. Young people’s needs are not confined to criminal justice or care placements. It is crucial to apply policies and practices across all types of institution, and to break down the artificial barriers between policy on criminal justice, health and social welfare. The evidence also strengthens the case for long term policy thinking in which young people are seen as beginning a life journey rather than merely crossing the boundary into a notional adulthood. Policy should be framed by a lifetime vision for children leaving institutional care, not by immediate palliation. Otherwise too many will continue to face the unacceptable prospect of a deadly despair.
Rory Corbett and Natalie Mazin are studying at the University of Surrey, having been research assistants at the Centre for Crime and Justice Studies where Dr Roger Grimshaw is Research Director. Paul Bebbington is Emeritus Professor of Psychiatry, University College, London
References
Bebbington, P., Bhugra, D., Brugha. T., Singleton, N., Farrell, M., Jenkins, R., Lewis, G., and Meltzer, H. (2004), ‘Psychosis, Victimisation, and childhood disadvantage: Evidence from the second British National Survey of Psychiatric Morbidity’, The British Journal of Psychiatry, 185, pp. 220-226.
Berlin, M., Vinnerljung., B., and Hjern, A. (2011), ‘School performance in primary school and pyschosocial problems in young adulthood among care leavers from long term foster care’, Children and Youth Services Review, 33, pp. 2489-2497.
Bruskas, D. (2008), ‘Children in Foster Care: A Vulnerable Population at Risk’, Journal of Child and Adolescent Psychiatric Nursing, 21(2), pp. 70–77.
Pecora, P., Williams, J., Kessler, R., Downs, A., O’Brien, K., Hiripi, E., and Morello, S. (2003), Assessing the effects of foster care: Early results from the Casey National Alumni Study, Seattle, WA: Casey Family Programs.
Pecora P., Kessler, R., O’Brien, K., White, C., Williams, J., Hiripi, E., English, D., White, J., and Herrick, M. (2006), ‘Educational and employment outcomes of adults formerly placed in foster care: Results from the Northwest Foster Care Alumni Study’, Children and Youth Services Review, 28, pp. 1459–481.
Pilowsky, D., and Wu, L-T. (2006), ‘Psychiatric symptoms and substance use disorders in a nationally representative sample of American adolescence involved with foster care’, Journal of Adolescent Health, 38(4), pp. 251-358.